Laparoscopic Roux-en-Y Gastric Bypass
 What is a Roux-en-Y Gastric Bypass?
What is a Roux-en-Y Gastric Bypass?
The laparoscopic Roux-en-Y gastric bypass operation has been performed since the late 1960’s to achieve significant weight-loss in people affected by severe obesity. The operation leads to weight-loss as a result of two different mechanisms:
- A small stomach pouch reduces the amount you can eat
- A small amount of intestine is bypassed leading to earlier release of gut hormones that make you feel less hungry
How is it performed?
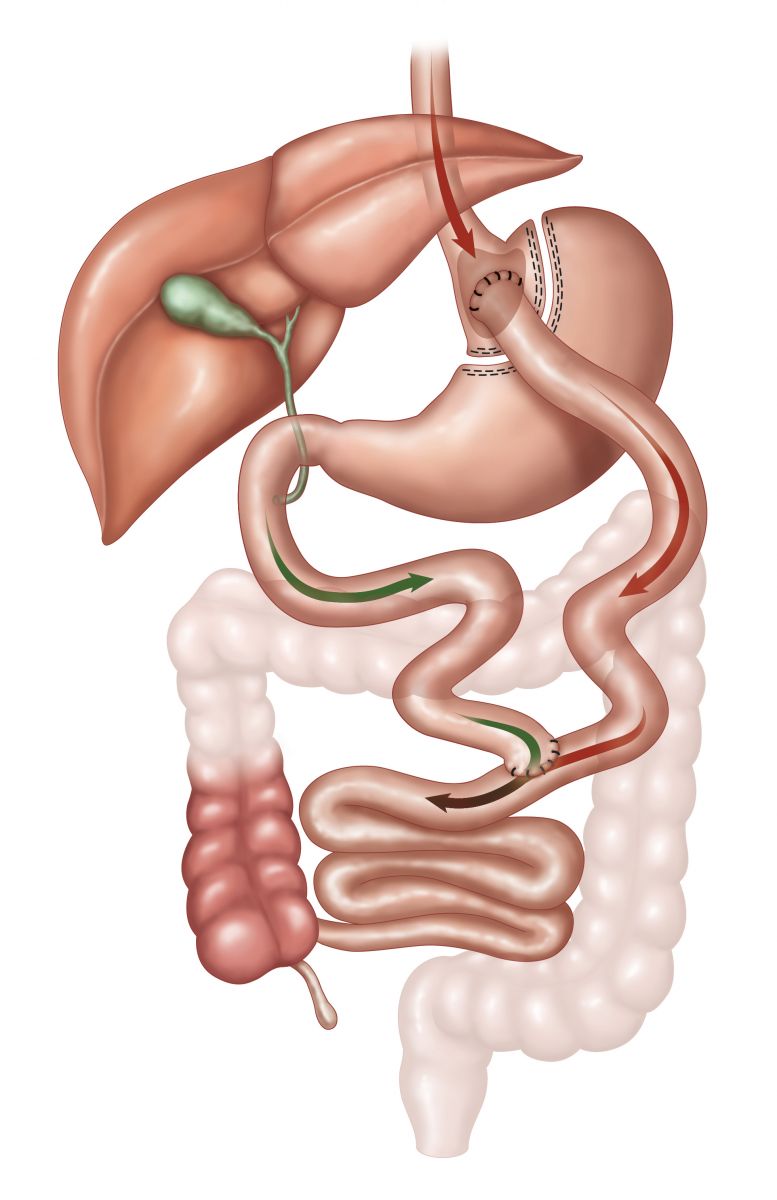
The surgery involves three basic steps:
- Dividing the stomach (about the size of a deflated regulation football) into two separate sections, creating a small pouch approximately the size of a man’s thumb and a larger excluded lower pouch (remnant of stomach)
- Bypassing a small portion of the small intestine
- Attaching the bypassed intestine (Roux Limb) to the proximal pouch
The laparoscopic roux-en-y gastric bypass can usually be done in two hours or less, but this will depend on many factors. Most patients will need to stay in the hospital for two to three days after their operation and should be ready to return to full activity within two weeks.
Click below to view the Gastric Bypass Procedure.
Advantages
- The average excess weight loss after the Roux-en-Y procedure is generally higher in a compliant patient than with purely restrictive procedures.
- One year after surgery, weight loss can average 77% of excess body weight.
- Studies show that after 10 to 14 years, 50-60% of excess body weight loss has been maintained by some patients.
- The “Short Intestinal Roux Limb” does not handle sugar or starches well so gastric bypass patients must limit their intake of sugary and starchy foods. If they don’t, they may experience something referred to as “Dumping Syndrome.” Usually 10-15 minutes after eating a sugary or starchy food, the individual who is “dumping” begins to experience many of the following symptoms:
- Sweating
- Flushing skin
- Rapid heart rate
- Dizziness
- Low blood pressure
- Abdominal pain
- Vomiting
- Diarrhea
- Shakiness
- Fainting
- Dumping typically lasts 30-45 minutes and then will go away. This gives the gastric bypass patient plenty of time to reflect on the food choice that they made that led to the dumping. For many people who have had a gastric bypass, dumping or the fear of dumping helps them make better food choices and stay away from foods that have tempted them in the past. Note-we view this as an advantage of gastric bypass surgery.
Risks
- Because the duodenum is bypassed, poor absorption of iron and calcium can result in the lowering of total body iron and a predisposition to iron deficiency anemia. This is a particular concern for patients who experience chronic blood loss during excessive menstrual flow or bleeding hemorrhoids. Women, already at risk for osteoporosis that can occur after menopause, should be aware of the potential for heightened bone calcium loss.
- Bypassing the duodenum has caused metabolic bone disease in some patients, resulting in bone pain, loss of height, humped back and fractures of the ribs and hip bones. All of the deficiencies mentioned above, however, can be managed through proper diet and vitamin supplements.
- A chronic anemia due to Vitamin B12 deficiency may occur. The problem can usually be managed with Vitamin B12 pills or injections.
- The bypassed portion of the stomach, duodenum and segments of the small intestine cannot be easily visualized using X-ray or endoscopy if problems such as ulcers, bleeding or malignancy should occur.